
Navigating thyroid health can be daunting, especially when faced with terms like follicular adenoma and carcinoma. Patients often worry about the implications of these diagnoses and the best course of action to ensure their health and well-being. Understanding the difference between follicular adenoma vs carcinoma is essential to make informed decisions about treatment options.
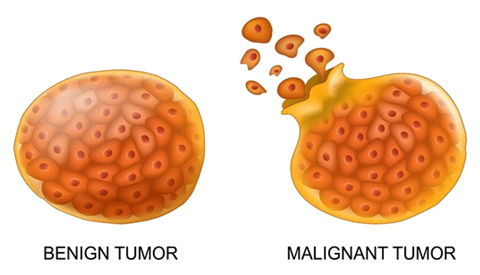
Both conditions involve growths on the thyroid gland. Follicular adenomas are generally benign thyroid nodules. On the other hand, follicular carcinomas are malignant and require more aggressive treatment.
According to Dr. Sandeep Nayak, a distinguished surgical oncologist in India and a leading expert in thyroid surgery, “Addressing thyroid nodules with precise evaluation helps distinguish between benign and malignant conditions, ensuring that patients receive the most appropriate care.”
Dr. Nayak is renowned for his expertise in thyroid cancer treatment in Bangalore. He offers advanced treatment options and specializes in minimally invasive techniques to help patients manage thyroid conditions.
Now, let’s understand the critical differences between follicular adenoma and carcinoma.
What is the Difference Between Adenoma and Carcinoma?
Follicular adenoma and carcinoma, although similar in some ways, differ fundamentally in their nature and behaviour. Understanding these differences is critical for accurate diagnosis and proper treatment. Here are the main distinctions:
Indications for Combined Thyroidectomy and Neck Dissection
A combined thyroidectomy and neck dissection may be indicated for several reasons, primarily associated with the management of thyroid cancer. Here are the key indications:
 Follicular Adenoma
Follicular Adenoma
 Follicular Adenoma
Follicular Adenoma- Nature:
- Benign tumor of the thyroid gland.
- Composed of follicular cells arranged in a microfollicular pattern.
- Does not invade surrounding tissues.
- Encapsulation:
- Encapsulated, meaning a fibrous capsule surrounds it.
- The capsule prevents the tumor from spreading to other tissues.
- Growth:
- Slow-growing and typically does not cause symptoms.
- May grow large enough to cause a noticeable nodule in the neck.
- Risk of Malignancy:
- Very low risk of transforming into carcinoma.
- Regular monitoring is usually sufficient to manage the condition.
Follicular Carcinoma
- Nature:
- Malignant tumor of the thyroid gland.
- Also composed of follicular cells but exhibits invasive properties.
- Capable of invading surrounding tissues and spreading to distant body parts.
- Invasion:
- Not encapsulated, or if a capsule is present, the tumor cells break through it.
- Can invade blood vessels and lymphatics, leading to metastasis.
- Growth:
- More aggressive and faster-growing than adenomas.
- Early detection and treatment are crucial to prevent spread.
- Risk of Spread:
- High risk of spreading to distant organs, including bones and lungs.
Now, let’s explore the diagnostic procedures for follicular adenoma and carcinoma.
How are Follicular Adenoma and Carcinoma Diagnosed?
Accurate diagnosis is crucial for effective treatment of thyroid conditions. Here are the primary diagnostic methods:
1. Clinical Examination:

Initial assessment by a healthcare provider, including palpation of the thyroid gland to detect lumps or abnormalities.
2. Imaging Studies:
Ultrasound:
 Helps visualize the thyroid gland and differentiate between solid and cystic nodules.
Helps visualize the thyroid gland and differentiate between solid and cystic nodules.
CT/MRI Scans: May be used to assess the extent of disease spread.
3. Fine-Needle Aspiration Biopsy (FNAB):
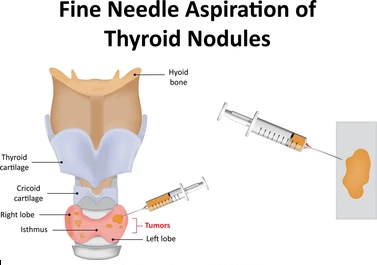 A minimally invasive procedure where a small sample of thyroid tissue is extracted and examined under a microscope.
A minimally invasive procedure where a small sample of thyroid tissue is extracted and examined under a microscope.
4. Blood Tests:
Thyroid Function Tests: To measure levels of thyroid hormones and TSH (Thyroid-Stimulating Hormone).
Molecular Testing: To identify genetic mutations associated with thyroid cancer.
5. Histopathological Examination:
Detailed microscopic analysis of biopsy samples to distinguish between benign and malignant cells.
Early diagnosis is critical. Consult an experienced specialist for accurate assessment. Book your appointment now.
Let’s explore the key symptoms that differentiate these conditions.
Key Differences in Symptoms Between Follicular Adenoma and Carcinoma
 Recognizing the symptoms is crucial for early intervention. Here are the primary symptoms:
Recognizing the symptoms is crucial for early intervention. Here are the primary symptoms:
- Follicular Adenoma:
- Often asymptomatic.
- Presence of a single, painless, and mobile thyroid nodule.
- Possible pressure symptoms if the lump grows large.
- No significant impact on thyroid function.
- Follicular Carcinoma:
- Persistent and possibly enlarging lump in the neck.
- Hoarseness or changes in voice.
- Difficulty swallowing or breathing.
- Persistent cough not related to a cold.
- Pain in the neck or throat.
- Swollen lymph nodes.
- Possible symptoms of hyperthyroidism or hypothyroidism.
Can a Follicular Adenoma Turn into a Carcinoma?
Follicular adenomas are generally benign thyroid tumors that arise from follicular cells. These growths are typically non-cancerous and do not spread to other body parts. However, there is a small risk that a follicular adenoma can undergo malignant transformation into follicular carcinoma.
This transformation involves changes at the cellular level that lead to aggressive behaviour, invasion of surrounding tissues, and potential spread to other organs. Thus, early and accurate diagnosis is crucial to managing this risk effectively. Regular monitoring and appropriate diagnosis are essential in distinguishing between benign and malignant nodules.
Let’s discuss about the treatment options available for managing these conditions.
How are Follicular Adenoma and Carcinoma Treated?
Treatment approaches vary based on whether the condition is benign or malignant. Here are the standard treatments:
Treatment of Follicular Adenoma
- Observation and Monitoring:
- Initial Approach: For asymptomatic or small follicular adenomas, regular monitoring with ultrasound and physical exams may be sufficient.
- Follow-Up: Periodic imaging and clinical evaluations help ensure that the adenoma remains benign and does not exhibit concerning changes.
- Surgical Removal:
- Indications for Surgery: Dr. Sandeep Nayak, an esteemed surgical oncologist in India, often recommends surgery if the adenoma causes symptoms, grows in size, or has suspicious features suggestive of malignancy.
- Types of Surgery: Depending on the size and characteristics of the adenoma, the procedure typically involves a lobectomy (removal of one lobe of the thyroid) or a total thyroidectomy (removal of the entire thyroid gland).
- Post-Surgical Care: Follow-up care includes monitoring thyroid hormone levels and ensuring complete removal of the adenoma.
Treatment of Follicular Carcinoma
- Surgical Intervention:
- Primary Treatment:
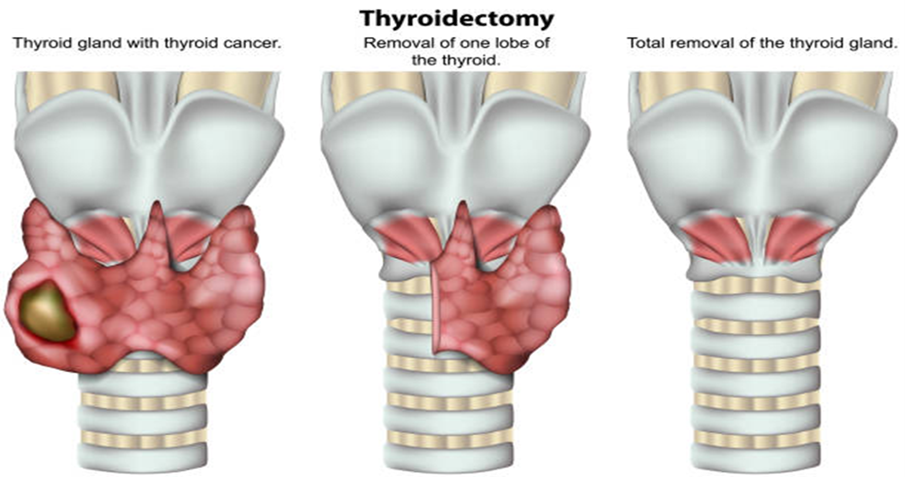
Total thyroidectomy is the standard treatment for follicular carcinoma. It involves the complete removal of the thyroid gland to ensure excision of all cancerous cells.
-
- Lymph Node Dissection: A thorough lymph node dissection may be performed in cases where cancer has spread to the lymph nodes.
- Radioactive Iodine Therapy:
- Post-Surgical Therapy: To destroy remaining cancer cells and prevent recurrence.
- Thyroid Hormone Therapy:

- Purpose: After thyroidectomy, patients typically require thyroid hormone replacement therapy to maintain normal thyroid function and suppress TSH (Thyroid-Stimulating Hormone) levels, which can stimulate any remaining cancer cells.
- Management: Regular blood tests to adjust medication dosages and monitor thyroid hormone levels.
- External Beam Radiotherapy:
- Use in Advanced Cases: If cancer has spread beyond the thyroid or is not fully removable.
- Targeted Therapy:
- For Advanced Disease: Drugs target specific pathways of cancer cells and inhibit their growth.
- Regular Follow-Up:
- Monitoring: After treatment, ongoing follow-up with imaging studies, thyroid function tests, and clinical evaluations is essential to detect any recurrence early and manage long-term health.
Conclusion
Understanding the differences between follicular adenoma and carcinoma is crucial for effective management and treatment. Timely diagnosis and intervention are vital to preventing complications and ensuring optimal outcomes.
Patients can manage their condition effectively and maintain their overall health with expert guidance and appropriate care. Consulting with a specialist is highly recommended for personalized advice and comprehensive care.
Explore the best treatment options for your condition. Schedule your appointment with a competent specialist now.
Frequently Asked Questions:
How does adenoma become carcinoma?
Adenoma can potentially become carcinoma due to genetic mutations or environmental factors, but this is rare.
What stage is carcinoma?
Carcinoma can vary in stage from I to IV. It depends on the size, location, and spread of the tumor.
Can follicular adenoma become cancerous?
While the risk is low, follicular adenomas can sometimes become cancerous. Hence, regular monitoring is vital.
What causes follicular adenoma?
The exact cause is unknown. However, factors like genetic mutations and radiation exposure may contribute.
What is the survival rate for follicular carcinoma?
The survival rate is high if detected early and treated appropriately. However, it can vary depending on the stage and spread of cancer.